
Spectral Power Distribution in Healthcare Lighting
Published by Lumega — Healthcare Lighting Division
The Limitations of Color Temperature as a Clinical Specification
When specifying lighting for healthcare facilities, the discussion typically centers on correlated color temperature (CCT) and illuminance. A psychiatric ward is typically specified at 300 lux and 3000K. A dementia unit at 500 lux and 2700K. A night corridor at 50 lux and 2200K.
This approach is inadequate—and in certain clinical contexts, downright counterproductive.
CCT describes a light source’s chromaticity relative to a theoretical blackbody radiator. It tells us where a light source is located on the Planck locus. It tells us nothing about the shape of its spectral power distribution—the actual energy emitted at each wavelength across the visible spectrum from 380 nm to 780 nm.
Two light sources can have an identical CCT of 2700K and yet produce radically different biological effects because their SPDs differ significantly in the short-wavelength range between 440 nm and 490 nm. This range—the blue channel of the visible spectrum—is not merely a contributor to visual appearance. It is the primary driver of the non-image-forming (NIF) photobiological response in humans.
ipRGC Photobiology: The Third Photoreceptor System
The discovery of intrinsically photosensitive retinal ganglion cells (ipRGCs) by Berson, Dunn, and Takao in 2002 fundamentally changed our understanding of how light interacts with human physiology beyond vision. Unlike rods and cones, ipRGCs express the photopigment melanopsin, with a peak spectral sensitivity at approximately 480 nm—firmly situated in the short-wavelength blue region.
ipRGCs project primarily to the suprachiasmatic nucleus (SCN) in the hypothalamus via the retinohypothalamic tract and directly regulate the central circadian clock. Secondary projections reach the pretectal nucleus (pupillary reflex), the lateral habenula (mood regulation), and the perihabenular nucleus, where there is emerging evidence of direct effects on mood disorders independent of the circadian system.
The clinical implications are significant. Melatonin suppression is mediated almost exclusively through ipRGC activation. Evening exposure to light with significant spectral energy at 480 nm suppresses melatonin onset, delays sleep onset, and reduces sleep efficiency. In older populations—where melatonin production is already significantly reduced—this effect is clinically significant. In dementia patients, where circadian rhythm disruption is both a symptom and an accelerator of neurodegeneration, it is critical.
Alertness and cortisol are acutely regulated via ipRGC-driven signals to the locus coeruleus and the hypothalamic-pituitary-adrenal axis. Short-wavelength light in the evening elevates cortisol, increases physiological arousal, and heightens agitation in populations with compromised neurological regulation—including those with dementia, acquired brain injury, and schizophrenia.
Mood regulation via the lateral habenula pathway is an area of active clinical research. The Norwegian psychiatric ward study published in *The Guardian* (March 2026) reported measurable improvements in treatment outcomes for psychosis and depression using integrated spectral lighting protocols — findings consistent with the emerging literature on ipRGC-mediated mood pathways that operate independently of circadian entrainment.
The Hidden Blue Spike Problem in Standard LED Technology
Modern phosphor-converted white LEDs—the technology underlying nearly all commercial LED fixtures—are manufactured by combining a blue InGaN die with a yellow phosphor layer. The phosphor converts part of the blue light emission into broad-spectrum yellow light. This combination produces the appearance of white light.
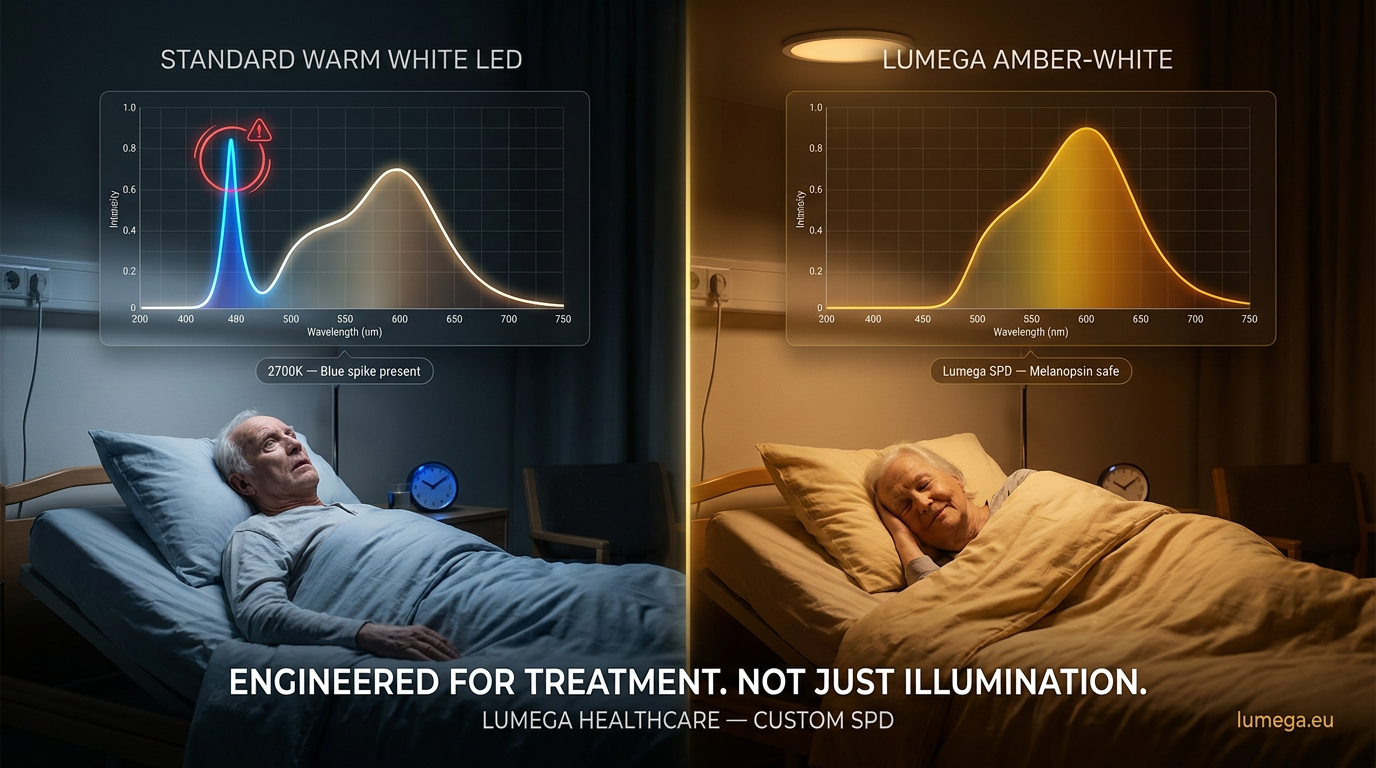
The fundamental problem is that phosphor conversion is never complete. All phosphor-converted white LEDs retain a residual emission peak from the underlying blue die, typically centered between 440 nm and 460 nm with a secondary contribution extending to 480 nm and beyond. This blue spike is a structural artifact of the manufacturing process—not a design choice.
In a luminaire specified for 2700K, the blue spike is visually imperceptible—the dominant impression is that of warm white light. However, spectrally, the ipRGC-activating component is present and biologically active. A 2700K phosphor-converted LED luminaire measured at 300 lux on the horizontal plane can provide a melanopic equivalent daylight illuminance (mEDI) of 80–120 lux mel—sufficient to produce significant melatonin suppression and circadian phase disruption when present in the evening environment.
For a dementia patient being prepared for bed at 9:00 p.m., this is not a marginal effect. It is a direct pharmacologically equivalent intervention, administered without clinical intent or control.
Lumegas Approach: Custom SPD Design
Lumega's manufacturing capabilities extend beyond its range of phosphor-converted white LEDs. We design luminaire spectral output using multi-channel LED arrays that enable clinical-grade SPD control across the entire visible spectrum.
Amber LED Arrays (590–620 nm)
Amber LEDs use a direct-emission InGaAlP die with peak emission in the 590–620 nm range. There is no blue die and no phosphor conversion. The spectral output contains zero energy below 500 nm—making it completely melanopsin-safe at any light level.
This technology forms the basis for the blue-light-blocking light therapy protocols used in research on the treatment of bipolar disorder at the University of Bergen and collaborating institutions. The clinical protocol from 2026 involves evening exposure to amber-spectrum lighting as a non-pharmacological intervention for mania prevention and circadian stabilization in patients with bipolar I disorder.
In our luminaire configurations, pure amber light sources are used for night lighting in psychiatric wards, dementia units, and ICU environments, where any suppression of melatonin is clinically unacceptable. At 10–30 lux horizontal illuminance, amber-spectrum luminaires provide sufficient visual task lighting for care staff while delivering a measured melanopic EDI below 1 lux mel.
Pink and Rose LED Assortments
Pink and rose LED assemblies combine direct-emission red and blue dies in specific ratios and bypass yellow phosphor conversion to produce a warm pinkish-white appearance. The blue LED contribution is selected and balanced to provide sufficient color rendering for clinical observation—accurate skin tone reproduction is a non-negotiable requirement in medical environments—while maintaining a reduced and spectrally suppressed blue peak.
Compared to equivalent CCT phosphor-converted light sources, well-designed pink LED arrays can reduce melanopic EDI by 40–60% at matched horizontal illuminance levels. In psychiatric settings, the reduced clinical harshness of pink light has been associated with reduced patient agitation and improved perception of environmental comfort—factors that are measurable on validated clinical scales, including the Pittsburgh Agitation Scale and the Cohen-Mansfield Agitation Inventory.

Amber-White Adjustable Assemblies
For environments that require full-spectrum color rendering combined with melanopsin-safe evening operation, Lumega designs adjustable amber-white luminaires that combine phosphor-converted warm white channels with direct-emission amber channels. At full white output, the luminaire delivers a standard warm white appearance with a CRI >90 for clinical daytime use. As the amber channel is proportionally increased throughout the evening transition, the spectral blue spike progressively diminishes until the 9:00 PM configuration delivers sub-threshold melanopsin stimulation while maintaining 200 lux horizontal illuminance.
This transition can be controlled automatically via Casambi or DALI-2 control systems, programmed to follow a facility-specific circadian protocol. The SPD profiles for each time of day can be customized by department or by room, with override capabilities for healthcare staff responding to urgent clinical needs.
The evidence base
The clinical evidence for spectral-specific light interventions in healthcare settings has reached a level of maturity that justifies their inclusion in facility design specifications.
A ClinicalTrials.gov-registered study (NCT05411822) demonstrated a reduction of more than 30% in agitated behavior among dementia patients within four weeks through a tailored light intervention using circadian-appropriate spectral profiles. The intervention was non-pharmacological and produced no side effects.
JAMA Psychiatry (2024) published findings confirming that light therapy—spectrally optimized for ipRGC stimulation—is an effective adjunctive treatment for non-seasonal depressive disorders, significantly expanding the evidence base beyond seasonal affective disorder.
A UC Davis study (2025) documented measurable reductions in cortisol, self-reported stress, and anxiety markers in participants exposed to amber-spectrum lighting compared to standard warm white lighting at matched light intensities.
The Norwegian Sanderud Hospital pilot (2026) demonstrated clinically meaningful improvements in treatment outcomes for depression and psychosis using integrated spectral lighting protocols—the first large-scale clinical facility to implement fully SPD-designed ward lighting as part of its treatment model.
Specification Considerations for Clinical Environments
Lighting designers, architects, and clinical engineers who specify lighting for healthcare environments should consider the following parameters in addition to conventional photometric specifications.
Melanopic Equivalent Daylight Illuminance (mEDI) is specified separately from photopic illuminance. CIE S 026/E:2018 provides the reference framework. Evening ward lighting should be designed to achieve an mEDI of less than 10 lux mel. Nighttime lighting should be less than 1 lux mel.
SPD documentation: Request full SPD curves from 380–780 nm for all specified luminaires—not just CCT and CRI. The blue channel contribution at 480 nm should be explicitly evaluated in relation to the intended clinical application.
Adjustment range: For circadian lighting systems, the full range of achievable melanopic EDI across the adjustment envelope is specified—not just the CCT range. A system that adjusts from 6500K to 2700K using phosphor-converted sources can only provide a 3:1 melanopic reduction ratio. A system that incorporates direct-emission amber channels can achieve a 100:1 or greater melanopic reduction ratio.
Third-party measurement: Specify that the delivered spectral output be verified by an independent third-party photometric measurement after installation. Lumega provides full SPD documentation and supports third-party measurement after installation as standard on all healthcare projects.

Conclusion
The science of light’s effects on human biology has advanced significantly beyond the color temperature scale. For clinical environments—psychiatric wards, dementia units, nursing homes, intensive care units, and secure facilities—the spectral composition of the light source is a clinical variable that deserves the same level of rigor as any other environmental intervention. Lumega’s position as a manufacturer with direct LED composition capabilities places us in a small group of lighting companies globally that can deliver truly evidence-based spectral design for healthcare environments. The combination of custom amber, pink, and amber-white LED compositions, Casambi or DALI-2 circadian control, and third-party SPD verification constitutes a complete clinical lighting solution—not a warm color temperature applied to a standard product line. We welcome technical inquiries from clinicians, healthcare architects, building engineers, and lighting designers working on projects where spectral precision is critical.
Contact: info@lumega.eu
Healthcare lighting: lumega.eu/healthcare
References are available upon request. All cited clinical data are derived from peer-reviewed publications and registered clinical trials.